

Your arm stops lifting properly one day.
You assume it is a muscle strain. You rest it. A week passes. Then a month. The stiffness gets worse instead of better. Reaching behind your back becomes impossible. Sleeping on that side wakes you up. Getting dressed in the morning is suddenly a painful negotiation with your own body.
This is frozen shoulder. And it is one of the most underdiagnosed and undertreated conditions in Chennai.
Most patients spend months cycling through painkillers, physiotherapy, and steroid injections, getting temporary relief each time, then returning to the same pain. Eventually, someone mentions manipulation under anaesthesia or capsular release surgery.
What almost nobody mentions is embolization.
A 45-minute outpatient procedure that targets the abnormal blood vessels driving chronic shoulder inflammation without cutting, without general anaesthesia, without weeks of surgical recovery.
This article explains exactly how it works, who it helps, and why it is changing how frozen shoulder is treated.
What is frozen shoulder embolization?
Frozen shoulder embolization, also called Musculoskeletal Embolization (MSKE) or Trans-Arterial Microembolization (TAME), is a minimally invasive catheter-based procedure. Tiny microscopic particles are delivered into the abnormal blood vessels supplying the inflamed shoulder joint capsule. Blocking these abnormal vessels reduces chronic inflammation, relieves pain, and improves movement without surgery, stitches, or general anaesthesia.
Understanding Frozen Shoulder: What Is Actually Happening Inside Your Joint

Frozen shoulder, the medical term is adhesive capsulitis, is not simply a stiff joint.
It is a condition where the capsule surrounding the shoulder joint becomes inflamed, thickened, and contracted. Scar tissue forms inside the capsule. The joint space shrinks. Movement becomes progressively restricted and painful.
What Causes Severe Shoulder Stiffness and Pain?
The shoulder joint is a ball-and-socket structure enclosed in a flexible capsule. That capsule is designed to allow the widest range of motion of any joint in the body.
When the capsule becomes inflamed from injury, prolonged immobility, post-surgical changes, or without any obvious trigger, a cycle begins:
- Inflammation thickens the capsule lining
- Thickening restricts fluid movement within the joint
- Restriction causes pain with movement
- Pain causes the patient to move less
- Reduced movement accelerates capsule contraction further
The result is a joint that progressively loses range of motion while pain increases, particularly at night when inflammatory activity peaks.
The 3 Stages of Frozen Shoulder
Understanding these stages helps you know where you are and what treatment is most appropriate.
The Freezing Phase (3 to 9 months)
- Gradual onset of shoulder pain
- Pain worsening at night often wakes the patient
- Range of motion begins to reduce
- Shoulder feels increasingly stiff after rest
- This is the inflammatory stage, where most active abnormal vessel growth occurs
The Frozen Phase (9 to 16 months)
- Pain may plateau or slightly reduce
- Stiffness is now the dominant problem
- Significant loss of movement in all directions
- Daily activities, such as dressing, reaching overhead, and driving, become consistently difficult
- Scar tissue formation is maximal at this stage
The Thawing Phase (12 to 24 months)
- Spontaneous gradual improvement begins
- Range of motion slowly returns
- Can take up to 3 years for full resolution in some patients
- Many patients never fully recover without intervention
The critical point most patients miss: Frozen shoulder can last 2 to 3 years without treatment. Even in the thawing stage, many patients retain permanent restriction. Waiting it out is not a neutral decision; it is choosing years of pain and functional limitation.
Why Diabetics and Women Face a Higher Risk
Two groups are significantly over-represented in frozen shoulder patients.
Diabetics:
- Both Type 1 and Type 2 diabetes increase frozen shoulder risk by 3 to 5 times compared to the general population
- High blood sugar promotes abnormal collagen formation in the joint capsule
- Glycation sugar molecules binding to proteins stiffens the capsule tissue directly
- Diabetic frozen shoulder tends to be more severe and longer-lasting
Women aged 40 to 60:
- Hormonal changes during perimenopause affect connective tissue elasticity
- Oestrogen reduction increases susceptibility to capsular inflammation
- Women make up approximately 70 per cent of frozen shoulder cases in clinical studies
Key Takeaway: Frozen shoulder is not a vague musculoskeletal complaint. It is a defined inflammatory condition with specific stages, specific risk groups, and a timeline measured in years, not weeks. Early effective treatment changes that timeline dramatically.
The Root Cause of the Pain: What Is Neovascularisation?
This is the part of frozen shoulder that most treatments miss entirely.
How Abnormal Blood Vessels Grow Inside Your Joint Capsule
When the shoulder capsule becomes inflamed, the body responds by growing new blood vessels into the area to support the inflammatory and repair process. This is called neovascularisation, the growth of abnormal new vessels where they should not exist.
These vessels are not normal. They are:
- Thinner and more fragile than normal vessels
- Accompanied by nerve fibres, which is why they cause pain
- Concentrated in the rotator interval and anterosuperior capsule, the areas most associated with frozen shoulder pain
- Self-perpetuating, they promote ongoing inflammation that encourages further vessel growth
This abnormal vessel network is the primary driver of the chronic, deep, night-time pain that characterises frozen shoulder in its active inflammatory phase.
It is also the direct target of embolization.
Why Traditional Painkillers Fail to Stop Chronic Joint Inflammation
Painkillers, such as NSAIDs, paracetamol, and opioids, reduce pain signal transmission. They do not reduce the abnormal vessel network, causing the inflammation.
This is why:
- Relief is temporary; the vessels remain active when the medication wears off
- Dosage requirements increase over time as chronic pain sensitisation develops
- Long-term NSAID use carries gastrointestinal and cardiovascular risk
- The underlying inflammatory process continues progressing regardless of pain management
Steroid injections reduce inflammation more effectively than oral medication, but again, temporarily. The abnormal vessels remain. Inflammation resumes when the steroid effect fades, typically within 6 to 12 weeks.
Key Takeaway: Painkillers and steroid injections manage the symptoms of frozen shoulder without addressing the abnormal vessel network that is producing the inflammation. Embolization addresses the network itself, which is why its effects are sustained rather than temporary.
What Is Frozen Shoulder Embolization?
Embolization for frozen shoulder is a direct application of interventional radiology principles to musculoskeletal inflammatory pain.
The Science Behind Musculoskeletal Embolization (MSKE)
MSKE was first developed for other musculoskeletal conditions, including knee arthritis and lateral epicondylitis, before being applied to frozen shoulder.
The principle is consistent across all applications:
Abnormal neovascularisation drives chronic inflammation. Blocking the blood supply to those abnormal vessels while sparing normal tissue reduces inflammation at the source. Pain decreases. Function improves. And unlike steroid injections, the effect is sustained because the vessel network itself has been reduced rather than temporarily suppressed.

Research from Japan, where MSKE was pioneered by Dr Okuno, has demonstrated consistent results across multiple musculoskeletal applications. Frozen shoulder studies show pain reduction of 70 to 80 per cent at 12 months in patients treated during the active inflammatory phase.
How Microscopic Beads Block Pain at the Source
The microspheres used in embolization are:
- 75 to 150 microns in diameter, smaller than a grain of sand
- Made from biocompatible materials designed to remain stable in the body
- Calibrated to specifically block small abnormal vessels too large to enter normal capillaries
- Non-toxic and non-reactive, with no systemic medication effect
When delivered into the abnormal shoulder vessels, these microspheres lodge in the feeding arteries of the neovascular network. Blood flow stops. The inflammatory supply is cut. The network begins to regress.
A Step-by-Step Guide to the 45-Minute Outpatient Procedure
Before the procedure:
- MRI of the shoulder confirms frozen shoulder diagnosis and stage
- Rules out rotator cuff tears or other structural issues requiring surgical management
- No general anaesthesia, local anaesthesia, and mild conscious sedation
- Patient remains awake and comfortable throughout
During the procedure:
- Small 2mm puncture in the elbow crease or wrist
- Catheter guided through the arterial system toward the shoulder under live X-ray imaging (DSA)
- Contrast dye injected maps the abnormal vessel pattern in the shoulder capsule
- Microspheres delivered into the specific abnormal vessels identified
- Normal blood supply to the shoulder muscles and joint preserved throughout
- Procedure time: 45 to 60 minutes
After the procedure:
- 2 to 3 hours monitored rest
- Mild shoulder soreness and warmth for 24 to 48 hours normal inflammatory response
- Same-day discharge
- Arm movement encouraged from day 1
- Return to desk work: 1 to 2 days
- Physiotherapy initiated within 1 week of pain reduction makes exercises significantly more effective
Key Takeaway: MSKE for frozen shoulder is a 45-minute outpatient procedure targeting the root cause of chronic shoulder inflammation. Same-day discharge. No general anaesthesia. Back to desk work within 2 days. Physiotherapy becomes effective rather than painful after the inflammation has reduced.
Why Embolization Is the Ultimate Frozen Shoulder Surgery Alternative

Embolization vs Manipulation Under Anaesthesia (MUA)
MUA involves placing the patient under general anaesthesia and forcibly moving the shoulder to break up the adhesions restricting movement.
The problems with MUA:
- Requires general anaesthesia and its associated risks
- Forcible manipulation carries the risk of labral tears, fractures, and rotator cuff damage
- Does not address the underlying neovascularisation driving inflammation
- Significant post-procedure pain, the capsule has been forcibly stretched
- Results are variable; some patients improve significantly, others see limited long-term benefit
- Physiotherapy immediately after is extremely painful, limiting effective rehabilitation
How embolization compares:
- Local anaesthesia only, no general anaesthesia risk
- No mechanical force on the shoulder, zero fracture or tissue tear risk
- Targets the inflammatory driver directly
- Mild soreness rather than severe post-procedure pain
- Physiotherapy after embolization is significantly more comfortable patients can participate effectively
Why Arthroscopic Capsular Release May Not Be Necessary
Arthroscopic capsular release involves keyhole surgery to cut the contracted capsule and allow the joint to move freely.
It works, but it comes with surgical requirements:
- General or regional anaesthesia
- Operating theatre time
- 1 to 3 days hospital stay
- 6 to 12 weeks of intensive physiotherapy
- Surgical risks: infection, nerve injury, and shoulder instability
For patients in Stage 2 frozen shoulder with severe structural contracture, capsular release may be the right answer. But for patients in Stage 1 to early Stage 2, where inflammation rather than structural contracture dominates embolization addresses the active disease process without any surgical intervention.
Zero Surgical Incisions: The Endovascular Advantage
The single most important practical difference:
Embolization requires a 2mm puncture. Nothing else touches the shoulder.
The procedure is performed through a tiny 2 mm puncture, eliminating the need for surgical incisions, stitches, wound care, or visible scarring. Because the shoulder itself is never opened, the risk of wound-related infection is also significantly reduced.
The entire intervention happens through the vascular system, guided by live imaging, reaching the shoulder from inside.
Key Takeaway: MUA and capsular release both require anaesthesia and carry procedural risks specific to forcible or surgical shoulder intervention. Embolization approaches the problem through the vascular system entirely, with no mechanical force, no incision, and no surgical risk to the shoulder itself.
Comparing Non-Surgical Treatments for Shoulder Pain
| Factor | Embolization (MSKE) | Cortisone Injection | PRP Injection | Physiotherapy alone |
| Targets the root cause | Yes, abnormal vessels | Partial reduces inflammation temporarily | Partial promotes healing | No |
| Anaesthesia | Local + mild sedation | None | None | None |
| Procedure time | 45–60 minutes | 5–10 minutes | 10–15 minutes | Ongoing sessions |
| Duration of relief | 12+ months sustained | 6–12 weeks typically | Variable 3–6 months | Symptom dependent |
| Pain during treatment | Minimal | Brief injection pain | Brief injection pain | Often significant |
| Effective in all stages | Stages 1 and 2 are best | All stages | Stage 1 and 2 | All stages |
| Enables physiotherapy | Yes significantly | Temporarily | Partially | Self-contained |
| Evidence base | Growing consistent results | Strong well established | Moderate | Strong |
| Suitable for diabetics | Yes | Caution raises blood sugar | Yes | Yes |
Cortisone Injections vs Shoulder Embolization
Cortisone injections work. They are the most commonly used treatment for frozen shoulder after physiotherapy fails.
The limitation is duration. The steroid effect wanes within 6 to 12 weeks. The underlying neovascularisation is not addressed. Inflammation returns. A second injection provides less relief than the first. A third, less still.
Repeated steroid injections also carry a cumulative risk of cartilage thinning, tendon weakening, and blood sugar elevation in diabetic patients specifically.
Embolization does not wear off in the same way. It reduces the vessel network itself, which is why sustained 12-month results are consistently documented.
PRP Treatment vs Embolization Which Works Faster?
PRP (Platelet-Rich Plasma) involves injecting concentrated growth factors from the patient’s own blood into the affected joint. It promotes tissue healing and reduces inflammation through biological signalling.
PRP has shown benefit for frozen shoulder, but results are variable, and its mechanism is indirect. Growth factors encourage healing but do not directly eliminate the abnormal blood vessel network (neovascularisation) that drives chronic inflammation.
Frozen shoulder embolization is an advanced form of Arterial Injection Treatment for Chronic Joint Pain, using image-guided catheter techniques to precisely target the abnormal blood vessels responsible for persistent pain. Unlike PRP, embolization works by reducing blood flow to these abnormal vessels, addressing the source of inflammation rather than simply promoting tissue repair.
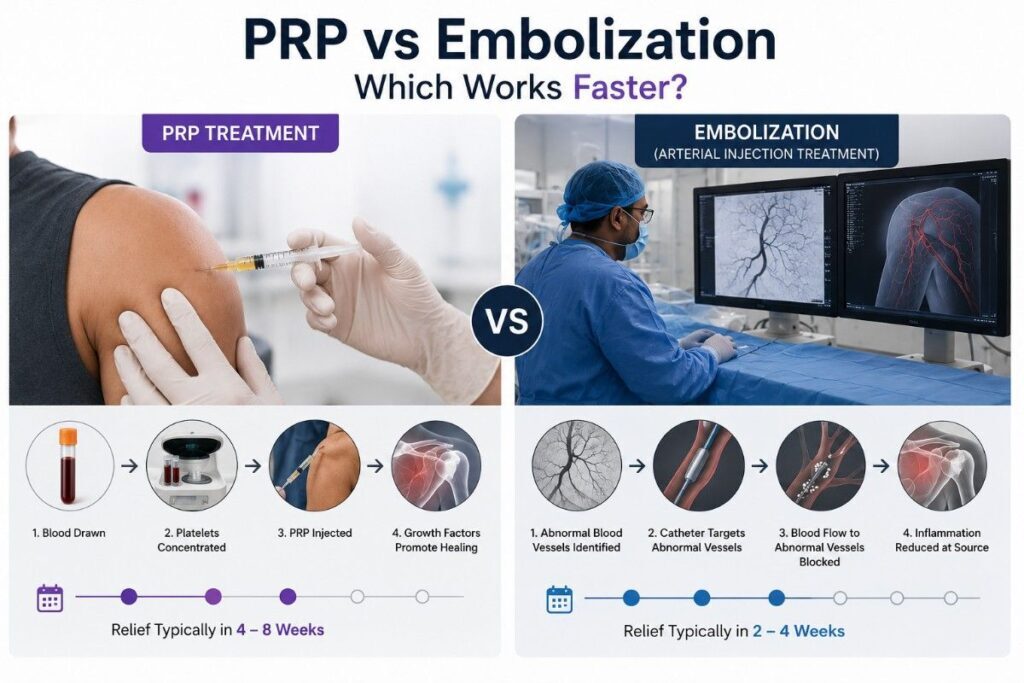
As a result, embolization often provides faster and more sustained symptom relief. Patients typically notice meaningful pain reduction within 2 to 4 weeks after embolization, compared with 4 to 8 weeks for PRP.
Why Physiotherapy Becomes Pain-Free Post-Embolization
This is one of the most practically important outcomes of embolization and one that is often underappreciated.
Physiotherapy for frozen shoulder is effective, but it requires the patient to move through pain. Many patients cannot tolerate the exercises needed to restore the range of motion because inflammation makes movement unbearable.
After embolization:
- The inflammatory driver is reduced
- Pain during movement decreases significantly
- Physiotherapy exercises become tolerable, then comfortable
- Range of motion returns faster because rehabilitation can progress without the pain barrier
Embolization and physiotherapy work synergistically. Embolization creates the conditions in which physiotherapy can actually work.
Key Takeaway: Embolization outperforms cortisone injections on duration and outperforms PRP on speed. More importantly, it makes physiotherapy effective by removing the pain barrier that prevents rehabilitation from progressing.
Recovery and Success Rates: What Patients Can Expect
Walk Out the Same Day Immediate Post-Procedure Protocol
Day of procedure:
- 2 to 3 hours rest in recovery
- Arm movement encouraged a gentle range of motion from hour 1
- Mild shoulder warmth and soreness are expected and normal
- Discharged same day
- Can travel home independently in most cases
Days 1 to 3:
- Soreness peaks at 24 to 48 hours managed with standard oral pain relief
- Light daily activity resumes immediately
- No immobilisation or sling required
- Desk work from day 1 to 2
Week 1 to 2:
- Pain begins to reduce noticeably
- Physiotherapy was initiated significantly more comfortably than pre-embolisation
- Sleep quality improves as night pain reduces
- Range of motion exercises progress faster without pain, limiting participation
When Will the Range of Motion and Internal Rotation Return?
Range of motion returns progressively, not immediately.
- Weeks 2 to 4: External rotation and forward flexion improve noticeably
- Month 2 to 3: Reaching overhead and across the body becomes comfortable
- Months 3 to 6: Internal rotation is the most restricted movement in frozen shoulder, and progressively recovers
- Months 6 to 12: Most patients achieve near full or full range of motion with consistent physiotherapy
The critical factor: physiotherapy participation post-embolization is the primary determinant of range of motion recovery speed. Pain reduction from embolization enables full physiotherapy engagement, which drives the motion return.
Clinical Success Rates for Long-Term Pain Relief
Published data from MSKE studies for shoulder conditions:
- 70 to 80 per cent of patients report significant pain reduction at 12 months
- Night pain, the most disabling symptom, shows the most consistent improvement
- Patient-reported outcome measures show sustained improvement at 24 months
- Repeat embolization is possible if needed without surgical risk accumulation
A 2021 study in Cardiovascular and Interventional Radiology reported VAS pain scores dropping from an average of 7.8 pre-procedure to 2.1 at 12 months in frozen shoulder patients treated with MSKE.
Key Takeaway: Embolisation produces 70 to 80 per cent sustained pain reduction at 12 months. Night pain, the most debilitating frozen shoulder symptom, responds most consistently. Range of motion recovery depends on post-procedure physiotherapy engagement, which is made possible by removing the pain barrier.
Choosing the Best Doctor for Frozen Shoulder Near Me
Why You Should Consult an Interventional Radiologist First
Most frozen shoulder patients see an orthopaedic surgeon first. This is understandable; shoulder pain feels like a musculoskeletal problem.
But orthopaedic surgeons offer orthopaedic solutions. Injections. Manipulation. Surgery. They do not perform embolization because embolization is a vascular intervention requiring catheter skills and DSA imaging expertise.
An interventional radiologist brings:
- Catheter-based procedural expertise
- Live X-ray (DSA) imaging capability
- Experience mapping and blocking abnormal vessel networks
- A non-surgical mindset treatment through the vascular system first
If you have been told your frozen shoulder needs MUA or capsular release and you are in Stage 1 or early Stage 2 one consultation with an interventional radiologist before surgery changes what you know your options are.
Frozen Shoulder Embolization at Dr Ravindran’s IR Clinic in Chennai
For patients searching for the best doctor for frozen shoulder near me in Chennai, the conversation should start with an interventional radiologist who performs MSKE.
Dr Ravindran, an Endovascular and Interventional Radiologist at Gleneagles Hospital, Veejay Towers, Velachery, Chennai, Tamil Nadu 600042, performs musculoskeletal embolisation as part of a comprehensive non-surgical treatment approach. Every case begins with an MRI assessment to confirm frozen shoulder stage, rule out structural pathology requiring surgery, and confirm MSKE suitability.
The assessment and procedure are both available at irdoctor in, where the principle is consistent across all conditions treated: surgery is the last option, not the first.
Key Takeaway: Frozen shoulder embolization requires an interventional radiologist, not an orthopaedic surgeon. If your current treatment plan involves MUA or capsular release and you have not consulted an IR specialist, you have not seen all your options yet.
Frequently Asked Questions
Published MSKE studies report 70 to 80 per cent pain reduction at 12 months in frozen shoulder patients. Night pain, the most disabling symptom, shows the most consistent and earliest improvement. A 2021 study in CardioVascular and Interventional Radiology reported VAS pain scores dropping from 7.8 to 2.1 at 12 months. Results are most consistent in Stage 1 and early Stage 2 frozen shoulder.
Steroid injections elevate blood sugar significantly, sometimes for 1 to 2 weeks after each injection. For diabetic patients with already challenging glucose management, this is a meaningful clinical concern. Repeated steroid injections compound this risk. Embolization does not affect blood sugar, has no systemic medication effect, and is therefore a safer long-term option for diabetic frozen shoulder patients specifically.
A cortisone injection delivers anti-inflammatory medication into the joint, reducing inflammation temporarily until the steroid effect wears off. The abnormal vessels causing inflammation to remain. Embolization blocks those vessels, directly reducing the inflammatory supply at its source. Effects are sustained at 12 months rather than 6 to 12 weeks. Embolization does not require repeated procedures in the way that steroid injections typically do.
Yes. Embolization is particularly relevant for patients who have had multiple steroid injections with diminishing returns and have found physiotherapy too painful to complete effectively. These are the patients where the neovascular network is most established and most directly responsive to embolization. Previous failed conservative treatment is not a contraindication.
Stage 1, the freezing stage, produces the most dramatic results because the inflammatory and neovascular activity is at its peak. Stage 2, the frozen stage, also responds well, particularly for pain relief. Stage 3 thawing has the least evidence for embolization benefit because natural resolution is already occurring. Early intervention produces better outcomes; waiting until Stage 3 is not recommended.
Conclusion
Frozen shoulder can last 2 to 3 years without effective treatment. Even then, many patients never fully recover their range of motion.
The standard pathway physiotherapy, then injections, then MUA or surgery works for some patients. But it misses the root cause entirely. The abnormal blood vessel network driving chronic inflammation continues growing throughout.
Embolization addresses that network directly. 45 minutes. Local anaesthesia. Same-day discharge. Back to desk work in 1 to 2 days. Night pain the most debilitating symptom, responds within weeks. Physiotherapy becomes possible rather than punishing.
If you are in Stage 1 or early Stage 2 frozen shoulder, or if you have had multiple injections with diminishing returns, one embolization consultation changes what you know your options are.
You should not spend 2 years waiting for a shoulder to thaw when treatment is available today.
Book a frozen shoulder embolization assessment with Dr Ravindran, Interventional Radiologist at Gleneagles Hospital, Veejay Towers, Velachery, Chennai, Tamil Nadu 600042 , Chennai
+91 8190 907 908 | Learn About TAME

Comments are closed