

Bleeding after passing stools, persistent discomfort while sitting, and a heaviness that never quite goes away, these are the symptoms that drive most patients to finally seek piles treatment without surgery. Hemorrhoid artery embolization changes that equation entirely. This minimally invasive procedure treats Grade II and III haemorrhoids without a single surgical incision, without general anaesthesia, and without weeks of painful recovery.
This minimally invasive procedure treats Grade II and III haemorrhoids without a single surgical incision, without general anaesthesia, and without weeks of painful recovery. Consequently, more patients across Chennai now choose this image-guided approach over laser or open surgery.
This guide explains exactly how the procedure works, who qualifies for it, and what recovery looks like so you can make a fully informed decision before your next specialist appointment.
What Is Hemorrhoid Artery Embolization?
“Hemorrhoid Artery Embolization (HAE) is a minimally invasive, image-guided procedure in which an Interventional Radiologist uses a catheter to block the superior rectal arteries supplying blood to haemorrhoidal tissue, causing the haemorrhoids to shrink progressively without surgical removal, incision, or general anaesthesia.”
| 90% Symptom improvement rate at 12-month follow-up (Cardiovascular and Interventional Radiology, 2022) | 2–3 days average recovery after HAE vs. 2–4 weeks after surgical haemorrhoidectomy | 75% of adults experience haemorrhoids at some point (American Society of Colon and Rectal Surgeons) | 0% Risk of anal sphincter damage with HAE the most feared complication of open surgery |
What Are Piles and Why Does Treatment Feel So Difficult?

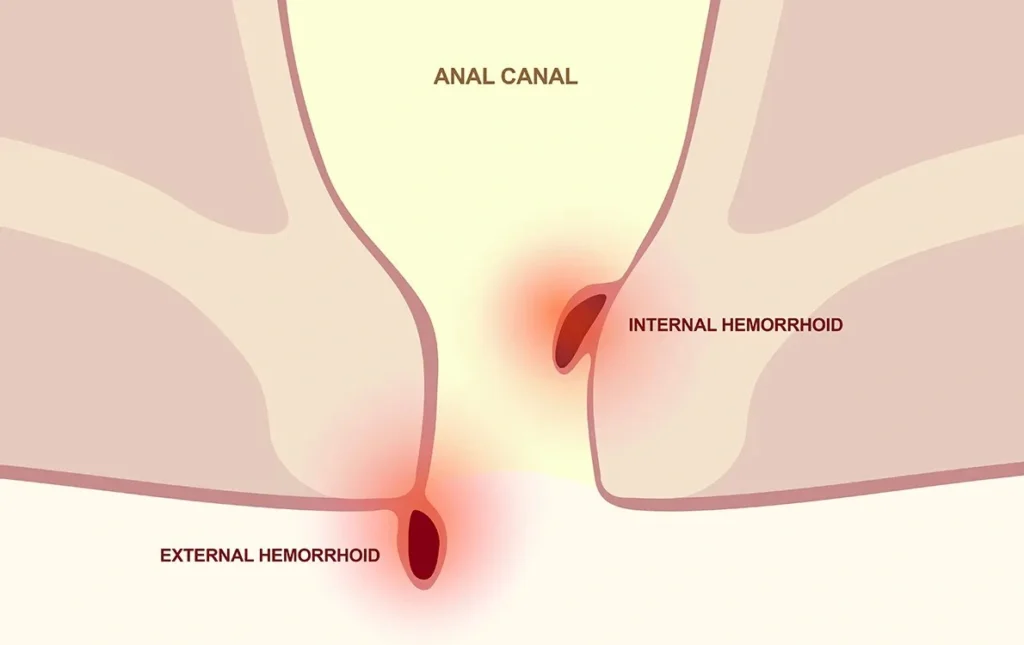
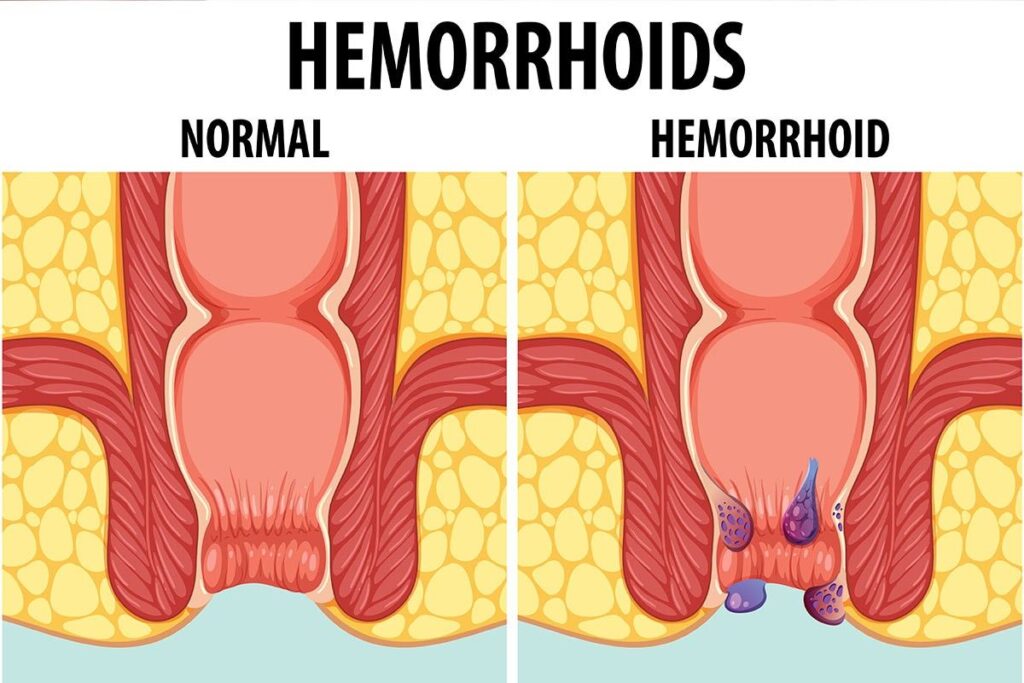
Haemorrhoids, commonly called piles, are enlarged vascular cushions in the lower rectum and around the anus. When the connective tissue supporting these cushions weakens, they engorge with blood, prolapse, bleed, and cause significant discomfort. Moreover, they worsen progressively without treatment, moving through four clinical grades from mild internal bleeding to permanent external prolapse.
Despite being extremely common, piles carry a social stigma that stops many patients from seeking help early. As a result, most patients arrive for assessment with Grade II or III haemorrhoids, the exact stage where HAE delivers its best results. Furthermore, the traditional assumption that surgery is inevitable drives avoidance when, in reality, most Grade II and III cases never need an operating theatre.
| Grade | What It Means | Typical Symptoms | Best Treatment |
|---|---|---|---|
| Grade I | Internal, no prolapse | Painless bleeding only | Diet and lifestyle changes |
| Grade II | Prolapse on straining, self-reducing | Bleeding + mild prolapse | HAE ideal candidate |
| Grade III | Prolapse requiring manual reduction | Bleeding + significant prolapse | HAE or laser |
| Grade IV | Permanently prolapsed | Constant prolapse + pain | Surgery required |
Pro Tip
Do not wait for bleeding to become heavy before seeking assessment. Painless rectal bleeding in the early stages, especially bright red blood on toilet paper, is Grade I or II haemorrhoid disease. Treating it at this stage is straightforward. Waiting until Grade III or IV narrows your non-surgical options significantly.
Key Takeaway
Most patients who seek piles treatment without surgery qualify for it — because most present at Grade II or III. The belief that surgery is inevitable stops many from seeking early assessment. However, early evaluation consistently opens the door to non-surgical options that later-stage patients can no longer access.
What Is Hemorrhoid Artery Embolization (HAE)?
HAE treats haemorrhoids by targeting their blood supply, not by cutting tissue out. An Interventional Radiologist guides a catheter through the arterial system to the superior rectal arteries that feed the haemorrhoidal cushions. Subsequently, the specialist injects tiny microspheres that reduce blood flow to the haemorrhoidal tissue. As a direct result, the tissue shrinks progressively over four to eight weeks.
Importantly, this approach addresses the root cause of haemorrhoidal disease rather than simply removing the visible consequence. Because no tissue is cut and no wound is created, patients experience minimal post-procedure pain and return to their routine within days rather than weeks.
People Also Ask: Is HAE the same as TACE used for liver tumours?
HAE uses the same image-guided embolization principle as TACE but targets the superior rectal arteries rather than hepatic vessels. Both procedures use catheter-based delivery of embolic particles under fluoroscopic guidance. HAE for haemorrhoids, however, is far less complex, carries minimal systemic risk, and applies to benign rather than malignant disease.
Key Takeaway
HAE does not remove haemorrhoids; it starves them of the blood supply that sustains their enlargement. Consequently, treated haemorrhoids shrink naturally over weeks, symptoms resolve progressively, and no surgical wound requires healing. This mechanism is precisely why recovery is measured in days, not weeks.
How HAE Works: The Step-by-Step Procedure
HAE takes place in an interventional radiology suite under local anaesthesia and mild sedation. Therefore, patients remain comfortable throughout and experience no general anaesthetic risk. The entire procedure typically takes between 45 and 60 minutes.
What Happens During the HAE Procedure?
- Pre-procedure imaging: The specialist reviews a CT angiogram to map the superior rectal artery anatomy before catheter navigation begins.
- Arterial access: A 2mm needle puncture in the wrist or groin provides access. No surgical incision, only a needle entry slightly larger than a blood test.
- Catheter navigation: Under real-time X-ray guidance, the specialist guides a thin catheter to the superior rectal arteries supplying the haemorrhoidal tissue.
- Microsphere injection: Tiny biocompatible microspheres pass through the catheter, lodging in the haemorrhoidal feeding vessels and reducing blood inflow immediately.
- Bilateral treatment: Crucially, the specialist treats both sides in one session, unlike surgery, which typically addresses one side at a time.
- Discharge: The catheter is removed, a small dressing applied, and most patients go home the same day.
Chennai-based Dr Ravindran Ramalingam — Endovascular & Interventional Radiologist demonstrates this catheter-guided approach in clinical practice by personally reviewing pre-procedure vascular imaging and performing bilateral superior rectal artery embolization in a single session. He illustrates how image-guided precision reduces both procedural time and post-treatment recurrence rates compared to surgical approaches that address haemorrhoidal tissue rather than its arterial supply.
Pro Tip Before Your HAE Appointment
Ask your specialist to confirm bilateral treatment in a single session. Some centres treat one side per visit, doubling recovery time and hospital attendance without clinical justification. Bilateral HAE in one session is the standard of care and the approach that delivers the highest symptom improvement rates at 12-month follow-up.
Key Takeaway
HAE achieves complete haemorrhoidal treatment through a 2mm puncture, no incision, no stitches, no wound care. Because the procedure addresses both sides simultaneously, patients leave with the full treatment done rather than awaiting a second session.
HAE vs Laser vs Surgery: Which Gives Faster Results?
Each treatment option delivers good outcomes for the right patient and the right grade. However, the speed of recovery, the level of post-procedure discomfort, and the risk profile differ considerably between them. Understanding these differences helps patients and specialists select the most appropriate option for each clinical situation.
| Feature | HAE | Laser | Open Surgery |
|---|---|---|---|
| Anaesthesia needed | Local + sedation | Local or spinal | General or spinal |
| Incision required | No 2mm puncture | Minimal | Yes multiple |
| Hospital stay | Same day / 1 night | Same day | 1–2 nights |
| Recovery time | 2–3 days | 5–10 days | 2–4 weeks |
| Post-procedure pain | Minimal | Mild–moderate | Significant |
| Sphincter damage risk | Zero | Very low | Small but present |
| Treats both sides | Yes one session | Usually one side | One or both |
| Success rate (12 months) | 90% | 85–90% | 95%+ |
| Best for | Grade II–III | Grade II–III | Grade III–IV |
People Also Ask: Is laser treatment for piles better than HAE?
Neither is universally better; a grade determines which is appropriate. For Grade II and III internal haemorrhoids, both deliver comparable 12-month success rates of 85–90%. However, HAE carries zero sphincter damage risk and achieves bilateral treatment in one session. Laser requires anaesthesia, a small procedure wound, and typically 5–10 days recovery versus 2–3 days for HAE.
Key Takeaway
HAE delivers the fastest recovery of the three treatment options, 2–3 days versus 5–10 days for laser and 2–4 weeks for surgery. Furthermore, it carries no sphincter damage risk and treats both sides in a single session. For Grade II and III haemorrhoids, it is the most patient-friendly non-surgical option currently available in Chennai.
Who Qualifies for Piles Treatment Without Surgery?
HAE works best for patients with Grade II or Grade III internal haemorrhoids who have not responded adequately to dietary and lifestyle modification. Additionally, it suits patients who want to avoid general anaesthesia, cannot afford extended recovery time, or have previously had surgery and experienced recurrence.
- Grade II internal haemorrhoids causing recurrent bleeding despite dietary measures
- Grade III haemorrhoids causing prolapse and discomfort that affects daily life
- Patients who have previously undergone rubber band ligation with recurrence
- Patients medically unfit for general anaesthesia due to cardiac, respiratory, or other conditions
- Patients who cannot take 2–4 weeks away from work or family responsibilities
- Patients with recurrent haemorrhoids after previous surgical haemorrhoidectomy
When Surgery Is Still Necessary
Surgery remains the appropriate choice for Grade IV haemorrhoids, those that are permanently prolapsed and cannot be manually reduced. Similarly, surgery suits patients with combined internal and large external haemorrhoids, thrombosed external haemorrhoids requiring acute intervention, or cases where tissue removal is necessary for diagnostic purposes.
Common Mistake
Assuming that a previous surgical haemorrhoidectomy rules out HAE for recurrent disease. In fact, recurrence after surgery, which occurs in 15–30% of cases, is one of the clearest indications for HAE. Because HAE targets the arterial supply rather than tissue, prior surgical scarring does not prevent the procedure from working effectively.
Key Takeaway
Grade II and III haemorrhoids are the ideal target for HAE, and together they represent the majority of patients seeking piles treatment in Chennai. If your haemorrhoid grade falls in this range, a surgical recommendation without discussing HAE first warrants a second opinion from an Interventional Radiologist.
Recovery After HAE: What Patients in Chennai Experience
Recovery after HAE is straightforward compared to both laser and surgical alternatives. Moreover, because the procedure creates no wound and requires no stitches, patients avoid the post-operative wound care that makes surgical recovery uncomfortable and time-consuming.
| Timeline | What to Expect | Activity Level |
|---|---|---|
| Day 1–2 | Mild pelvic discomfort, managed with standard analgesics. Small dressing on wrist/groin puncture site. | Rest light walking encouraged |
| Day 3–5 | Discomfort resolves significantly. Puncture site heals fully. Light activity resumes comfortably. | Desk work and driving resume |
| Week 2–4 | Haemorrhoids begin shrinking. Bleeding reduces noticeably. Prolapse symptoms ease progressively. | Full normal activity |
| Month 1–2 | Maximum haemorrhoidal shrinkage achieved. Most symptoms resolve. Follow-up review confirms treatment response. | Unrestricted |
| Month 6–12 | Sustained symptom relief in 90% of patients. Dietary fibre and hydration maintenance reduces recurrence risk. | Unrestricted |
Pro Tip After Your HAE Procedure
Increase dietary fibre to 25–30g daily and drink 2–2.5 litres of water throughout the day starting immediately after HAE. This single lifestyle change reduces the straining that originally drove haemorrhoidal development and therefore reduces your five-year recurrence risk significantly. Psyllium husk sachets dissolved in water are the most convenient and evidence-backed approach for Chennai patients.
People Also Ask: How long after HAE do haemorrhoids start shrinking?
Haemorrhoids begin shrinking within days of HAE as the blood supply diminishes. Noticeable symptom improvement, particularly reduction in bleeding, typically occurs within the first 2–4 weeks. Maximum shrinkage and full symptom resolution develop over 4–8 weeks. A follow-up review at 6–8 weeks confirms the treatment response and addresses any residual symptoms.
Key Takeaway
Most patients return to desk work within 2–3 days of HAE compared to 2–4 weeks after surgical haemorrhoidectomy. Because recovery is this rapid, HAE removes the practical barrier that causes many Chennai patients to delay piles treatment indefinitely. The procedure that seemed disruptive turns out to take less time than a long weekend.
Piles Specialist in Chennai — Dr. Ravindran Ramalingam
Dr Ravindran Ramalingam is an Endovascular and Interventional Radiologist at Gleneagles Health City, Perumbakkam, Chennai. He performs Hemorrhoid Artery Embolization as his primary non-surgical treatment for Grade II and III haemorrhoids, combining pre-procedure angiographic mapping with bilateral embolization in a single session to maximise treatment completeness.
Unlike surgical referral pathways where a colorectal surgeon assesses and treats, Dr. Ravindran’s approach integrates imaging assessment and interventional treatment under one specialist eliminating the delays and communication gaps that occur when imaging and treatment are separated across different clinical teams.
Frequently Asked Questions
How do I know whether I need HAE or surgery for my piles?
Grade determines the answer. A specialist clinical examination and proctoscopy confirm your haemorrhoid grade in one visit. Grade II and III internal haemorrhoids qualify for HAE. Grade IV haemorrhoids permanently prolapsed require surgery. Never agree to treatment before your grade is confirmed, because applying the wrong procedure to the wrong grade produces poor outcomes regardless of technique.
What makes hemorrhoid artery embolization different from rubber band ligation?
Rubber band ligation cuts off the blood supply to individual haemorrhoids one at a time by applying a tight band around the base of each. HAE reduces the arterial blood supply to all haemorrhoids simultaneously through the feeding arteries. As a result, HAE treats multiple haemorrhoids in one session, carries no risk of band slippage or post-banding bleeding, and suits larger Grade III haemorrhoids where banding is less effective.
Why is piles treatment without surgery not offered in most Chennai hospitals?
HAE requires an Interventional Radiologist with catheter-based vascular skills, a specialist not present in most general surgical departments. Consequently, most hospitals default to laser or surgical options simply because their team structure does not include IR expertise. Patients seeking HAE specifically should book with an Interventional Radiologist rather than a colorectal or general surgeon.
When can I return to work after hemorrhoid artery embolization?
Most patients return to desk work within 2–3 days of HAE. Physical or outdoor work typically resumes at day 5–7. There are no wound care requirements, no dressings to change, and no activity restrictions beyond avoiding heavy lifting in the first week. This recovery timeline is significantly faster than both laser (5–10 days) and open surgery (2–4 weeks).
Which piles treatment has the lowest risk of complications in Chennai?
HAE carries the lowest overall complication profile of the three main options. Specifically, it eliminates the risk of anal sphincter damage, the most serious complication of surgical haemorrhoidectomy and avoids the post-procedure wound infections seen after laser and open procedures. The only procedure-specific risk is arterial access site bruising, which resolves within 5–7 days.
Key Takeaways Piles Treatment Without Surgery
- HAE treats Grade II and III haemorrhoids without surgery, incision, or general anaesthesia by targeting the blood supply rather than removing tissue
- Recovery takes 2–3 days, significantly faster than laser (5–10 days) or open surgery (2–4 weeks)
- 90% symptom improvement at 12 months makes HAE clinically comparable to surgical options for appropriate grades
- Bilateral treatment in a single session is the standard confirm this before proceeding with any HAE provider
- Grade determines treatment always confirm your haemorrhoid grade before agreeing to any procedure
- HAE is performed exclusively by Interventional Radiologists not by colorectal or general surgeons
Conclusion: Piles Treatment Has Changed and Surgery Is No Longer the Default
For decades, patients with Grade II and III haemorrhoids in Chennai faced a choice between managing symptoms with creams and laxatives or accepting surgical intervention. HAE removes that false binary entirely. As a result, patients who previously delayed treatment out of fear of surgery now have access to a same-day procedure that delivers lasting relief with a 2–3 day recovery.
The first step is a specialist assessment to confirm your haemorrhoid grade. From there, a clear treatment recommendation, whether HAE, laser, or surgery, follows logically from your clinical picture rather than from institutional habit or default referral patterns.
You do not have to keep managing around piles. A straightforward assessment changes everything.
Ready to Explore Piles Treatment Without Surgery?
Book a consultation with Dr Ravindran Ramalingam, HAE Specialist, Gleneagles Health City, Chennai
📞 +91 8190 907 908 | Learn About HAE ↗
Medical Disclaimer: This article is for informational and educational purposes only. It does not constitute medical advice, diagnosis, or a treatment recommendation. All haemorrhoid management decisions should be made with a qualified medical specialist following clinical assessment.
Comments are closed