

Getting up three times a night to urinate is not aging gracefully.
Neither is standing at the toilet waiting for a stream that barely comes. The constant feeling that your bladder never fully empties makes every trip frustrating. And that sudden urgency, the kind that sends you rushing and sometimes not making it in time, affects confidence, sleep, and daily life in ways most men never discuss openly.
These are the daily realities of benign prostatic hyperplasia (BPH). Millions of Indian men over 50 are living with them right now. Many stay silent, assuming it is simply part of getting older. What most of them do not know is that an effective non-surgical solution exists, one that does not require general anesthesia, a hospital stay, or the sexual side effects that surgery carries.
The standard conversation goes like this: Try medication for a year or two. When that stops working, consider surgery. TURP. A procedure that passes instruments through the urethra, removes prostate tissue, and carries a well-documented risk of retrograde ejaculation, a permanent change to sexual function that most men are not fully counselled about before they consent.
There is a better conversation to have first.
What is Prostate Artery Embolization (PAE)?
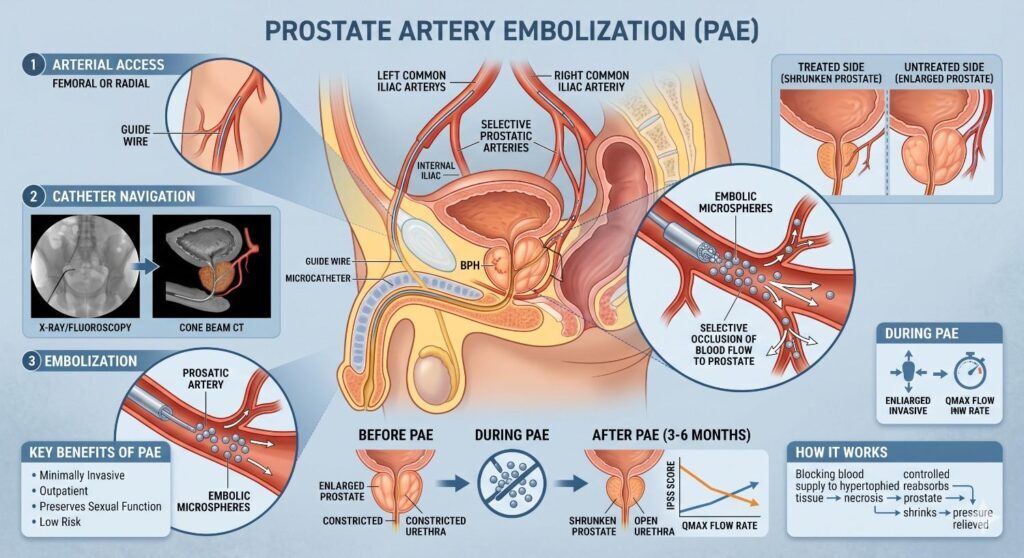
PAE is a minimally invasive procedure where tiny microspheres are delivered through a catheter into the arteries supplying the enlarged prostate. Blood flow to the prostate via artery embolization is reduced. The gland shrinks over 4 to 8 weeks. Urinary symptoms improve significantly without surgery, general anesthesia, or any instrument inserted through the urethra.
Understanding Benign Prostatic Hyperplasia What Is Actually Happening
BPH is not cancer. It is not dangerous in its early stages. But left untreated, it progressively worsens and eventually becomes a medical problem that cannot be ignored.
Why the Prostate Enlarges and How It Restricts Urine Flow
The prostate gland sits directly below the bladder and surrounds the urethra, the tube that carries urine out of the body.
In younger men, the prostate is roughly the size of a walnut, about 20 to 30 grams. As men age, the prostate grows. This is driven by hormonal changes, specifically the balance between testosterone and estrogen shifting over time.
The problem is anatomical:
- As the prostate enlarges, it compresses the urethra from all sides
- The compressed urethra restricts urine flow like squeezing a garden hose
- The bladder works harder to push urine through the restriction
- Over time, the bladder wall thickens from overwork
- Eventually the bladder becomes less efficient, unable to empty fully
The result is a progressive combination of obstructive and irritative urinary symptoms that worsen year by year.
Identifying the Signs From Weak Stream to Frequent Night Urination
BPH symptoms fall into two categories. Most men experience both simultaneously.
Obstructive symptoms caused by the physical blockage:
- Weak or slow urinary stream
- Difficulty starting urination standing and waiting
- Stream that stops and starts rather than flowing continuously
- Feeling that the bladder has not fully emptied after urinating
- Dribbling at the end of urination
- Straining required to initiate or maintain flow
Irritative symptoms caused by bladder overactivity:
- Frequent urination more than 8 times daily
- Nocturia: waking 2 or more times per night to urinate
- Urgency: sudden, difficult-to-defer need to urinate
- Urgency incontinence, not reaching the toilet in time
- Sensation of bladder fullness even immediately after urinating
The International Prostate Symptom Score (IPSS) measures these symptoms on a scale of 0 to 35. Scores above 20 indicate severe BPH. Most men seeking treatment score between 15 and 28.
When Does an Enlarged Prostate Become a Medical Emergency?
BPH progresses slowly, but some situations require urgent medical attention.
Go to the emergency department immediately if the following are true:
- You cannot urinate at all: acute urinary retention
- Severe lower abdominal pain with a visibly distended bladder
- Blood in the urine (hematuria), particularly with clots
- Kidney pain or fever alongside urinary symptoms suggesting infection has reached the upper urinary tract
Acute urinary retention, the complete inability to pass urine, requires emergency catheterization. It is not uncommon for BPH to progress without treatment. And once it happens, the window for non-surgical management narrows.
Key Takeaway: BPH starts as an inconvenience and ends as a medical emergency if untreated. The IPSS score above 20, nocturia more than twice per night, and progressively worsening flow are the signals that watchful waiting has reached its limit.
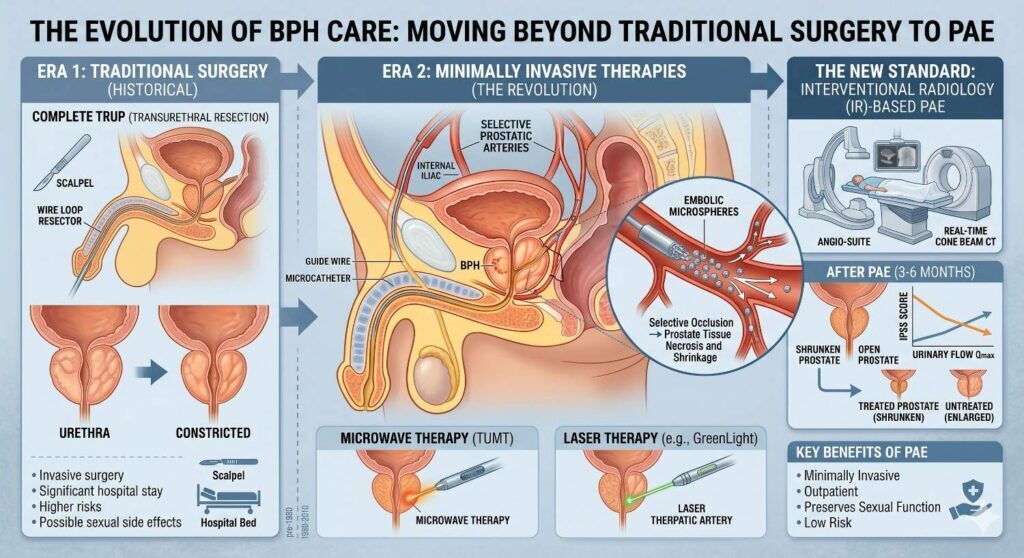
The Evolution of BPH Care: Moving Beyond Traditional Surgery
Why Long-Term BPH Medications May Not Be the Best Answer
Alpha-blockers tamsulosin and alfuzosin relax the prostate muscles and improve urine flow. 5-alpha reductase inhibitors, finasteride and dutasteride, reduce prostate size slowly over 6 to 12 months.
These medications work. For mild to moderate BPH, they are a reasonable first step.
But the limitations are real:
- Alpha-blockers: do not reduce prostate size. Symptoms return when medication stops. Side effects include dizziness, low blood pressure, and retrograde ejaculation in some patients.
- 5-ARI medications: take 6 to 12 months for a meaningful effect. Causes sexual side effects in 5 to 10 percent of men: reduced libido, erectile dysfunction, and ejaculatory changes. Some men experience persistent side effects even after stopping the medication.
- Combination therapy: more effective but doubles the side effect profile
- Neither medication type is curative: they manage BPH while the underlying gland continues to grow
For men with moderate to severe BPH, or those whose symptoms have progressed on medication, definitive treatment is the more appropriate conversation.
What Is TURP? The Realities of Transurethral Resection of the Prostate
TURP has been the gold standard surgical treatment for BPH for over 50 years.
It involves:
- General or spinal anaesthesia
- A resectoscope, a rigid instrument inserted through the urethra into the prostate
- Electrical current used to remove obstructing prostate tissue from the inside
- Hospital stay: 2 to 3 days
- Urinary catheter: required for 1 to 3 days post-procedure
- Return to normal activity: 2 to 4 weeks
TURP works well for improving urine flow. But the side effects are significant and poorly understood by most patients before they consent:
- Retrograde ejaculation, where semen travels backwards into the bladder rather than out, occurs in 50 to 75 percent of TURP patients. This is permanent.
- Erectile dysfunction occurs in approximately 10 to 15 percent of cases
- Urinary incontinence temporary in most cases and permanent in a small percentage
- Urethral stricture scarring of the urethra from instrumentation requires further treatment
Surgical Laser Procedures (HoLEP) vs. Non-Surgical Embolization
HOLEP, Holmium Laser Enucleation of the Prostate, is a more advanced surgical option. It removes more prostate tissue than TURP with a lower bleeding risk.
But HoLEP shares the fundamental limitation of all surgical approaches:
- General or spinal anaesthesia required
- Instrument inserted through the urethra
- A retrograde ejaculation rate similar to that of TURP, 50 to 75, occurs
- percent
- Hospital stay 1 to 2 days
- 2 to 4 weeks to return to full activity
The critical difference with PAE:
PAE approaches the prostate through the arterial system, not through the urethra. Nothing is inserted into the urinary tract. The sexual nerve pathways are not affected. Retrograde ejaculation risk is effectively zero.
| Factor | PAE | TURP | HoLEP |
| Anaesthesia | Local + mild sedation | General or spinal | General or spinal |
| Instrument through urethra | No, never. | Yes | Yes |
| Hospital stay | Same day | 2–3 days | 1–2 days |
| Urinary catheter post-op | Usually not needed | 1–3 days | 1–2 days |
| Retrograde ejaculation risk | Effectively zero | 65–90% | 75–90% |
| Erectile dysfunction risk | Very low | 10–15% | 5–10% |
| Return to normal activity | 2–5 days | 2–4 weeks | 2–4 weeks |
| Suitable for high surgical risk | Yes, specifically. | No | No |
| Suitable for very large prostate (>80g) | Yes, particularly. | Less effective | Yes |
Key Takeaway: TURP and HoLEP achieve good urinary symptom relief but carry a 50 to 90 percent retrograde ejaculation rate a permanent change most men are not fully counselled about before consenting. PAE achieves comparable urinary improvement without touching the urethra and without affecting sexual function.
What Is Prostate Artery Embolization: The Full Procedure Explained
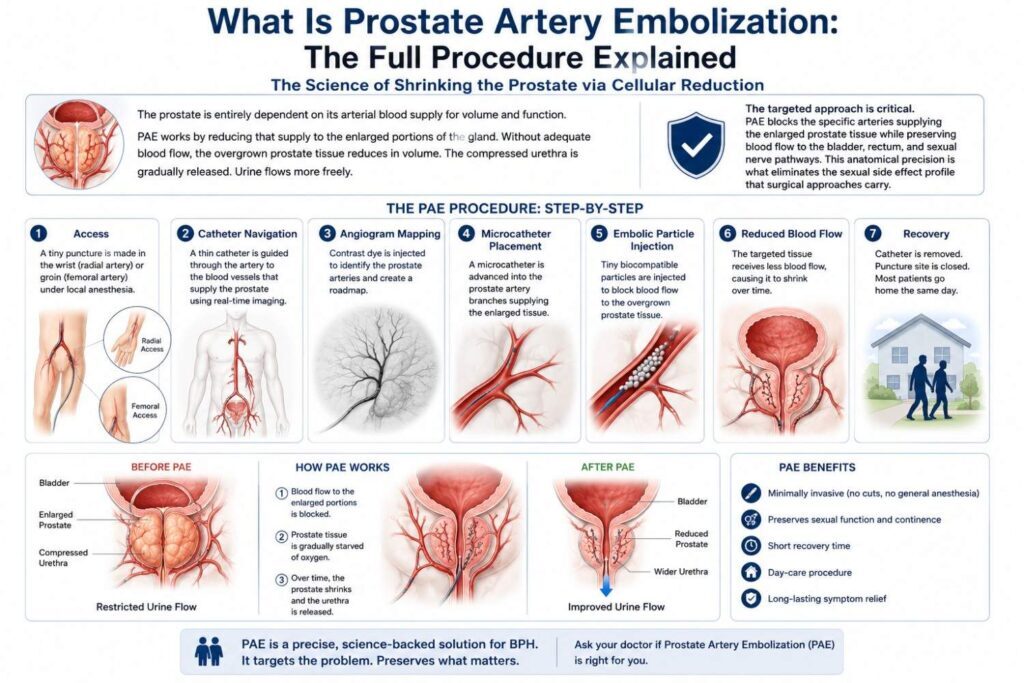
The Science of Shrinking the Prostate via Cellular Reduction
The prostate is entirely dependent on its arterial blood supply for volume and function.
PAE works by reducing that supply to the enlarged portions of the gland. Without adequate blood flow, the overgrown prostate tissue reduces in volume. The compressed urethra is gradually released. Urine flows more freely.
The targeted approach is critical. PAE blocks the specific arteries supplying the enlarged prostate tissue while preserving blood flow to the bladder, rectum, and sexual nerve pathways. This anatomical precision is what eliminates the sexual side effect profile that surgical approaches carry.
Step-by-Step: How the Procedure Works
Before the procedure:
- Prostate MRI or TRUS (transrectal ultrasound) confirms prostate size and anatomy
- Urine flow rate test (uroflowmetry) and post-void residual measurement establish baseline
- The IPSS score was documented and used for outcome comparison at follow-up
- No general anesthesia required, only local anaesthesia and mild conscious sedation
- Patient awake and comfortable throughout
During the procedure:
- 2 mm puncture in the wrist or groin; patient’s preference and anatomy guide the choice
- Catheter guided through the arterial system toward the prostate arteries under live X-ray imaging (DSA)
- Contrast dye injected creates a detailed map of the prostatic arterial anatomy
- Microcatheter advanced selectively into the arteries supplying the enlarged prostate tissue
- Tiny microspheres, 100 to 300 microns, are delivered to block these specific vessels
- Both sides treated in sequence during the same session
- Normal blood supply to surrounding structures preserved throughout
- Procedure time: 60 to 120 minutes depending on arterial anatomy complexity
After the procedure:
- 2 to 4 hours monitored recovery
- Mild pelvic discomfort and urinary urgency for 24 to 72 hours are expected and manageable
- Same-day discharge in the majority of cases
- No catheter required in most patients
- Return to desk work: 2 to 3 days
- Full normal activity: 5 to 7 days
Why Microsphere Technology Provides a Precise, Targeted Alternative
The microspheres used in PAE are:
- 100 to 300 microns in diameter calibrated for prostate arterial anatomy specifically
- Biocompatible: designed to remain stable permanently within the vessel
- Sized to block prostatic arterioles selectively too large to travel into normal capillary beds
- Non-toxic, no systemic medication effect
This precision is what makes PAE different from surgical approaches. The reduction in prostate volume happens from inside the arterial system guided by live imaging without any mechanical contact with the prostate, urethra, or surrounding sexual structures.
Key Takeaway: PAE reduces prostate volume by selectively blocking its arterial supply using microspheres delivered through a catheter from a wrist or groin puncture. Nothing enters the urethra. The sexual nerve pathways are untouched. The prostate shrinks over 4 to 8 weeks as its blood supply reduces.
Why PAE Is the Best Treatment for Enlarged Prostate Without Surgery
Zero Surgical Cuts Zero Instruments Through the Urethra
This single point changes everything for many patients.
TURP and HoLEP both require a rigid or flexible resectoscope passed through the urethra into the prostate. The urethra is not designed for this. The risks of stricture formation, infection, and post-operative incontinence all arise directly from this instrumentation.
PAE bypasses the urinary tract entirely. The prostate is reached through the arterial system. The urethra is never touched. The risks associated with urethral instrumentation do not apply.
Preserving Male Health: Why PAE Eliminates Retrograde Ejaculation Risk
Retrograde ejaculation where semen travels into the bladder rather than out occurs in 50 to 75 percent of TURP patients.
It happens because TURP removes the internal urethral sphincter, the muscular mechanism that prevents backward ejaculation. Once removed, this function cannot be restored.
PAE does not touch the sphincter. It does not touch the urethra. The ejaculatory mechanism remains anatomically intact. Published PAE studies consistently report retrograde ejaculation rates of less than 1 to 2 percent, effectively zero, compared to surgical alternatives.
For men under 65 who are sexually active, this difference is not minor. It is the single most important functional outcome difference between PAE and surgical BPH treatment.
Local Anaesthesia Only Built for Fast Recovery
The anesthesia difference matters beyond just comfort during the procedure.
General and spinal anesthesia carry risks, particularly for older patients, those with cardiac conditions, diabetics, and men on blood thinners. These are exactly the patients most likely to need BPH treatment.
PAE under local anesthesia:
- Eliminates general anaesthesia risk entirely
- Suitable for patients with significant cardiac history
- Safe for patients on anticoagulation with appropriate management
- No post-anaesthesia recovery time
- Patient can eat and drink immediately after
- Discharge the same day in most cases
Key Takeaway: PAE’s three core advantages over surgery no urethral instrumentation, zero retrograde ejaculation risk, and local anesthesia only, are not minor conveniences. There are clinically significant differences in safety, functional outcome, and recovery that every man with BPH deserves to understand before choosing a treatment.
Who Is a Candidate for PAE in Chennai
Why Very Large Prostates Over 80 Grams Are Ideally Suited for PAE
Surgical approaches for very large prostates are technically more demanding and carry higher complication rates. TURP for prostates over 80 grams has limited tissue removal capacity. Open prostatectomy, a major surgery, has historically been the alternative for very large glands.
PAE has no upper size limit in the same way. Studies consistently show strong outcomes for prostates in the 80 to 200 gram range. The larger the prostate, the more arterial supply it carries and the more dramatically blood flow reduction affects its volume.
Very large prostates are not a contraindication for PAE. For many interventional radiologists, they are the optimal indication.
Treating BPH Safely for High Cardiovascular Risk Patients
PAE is specifically suitable for patients who cannot safely undergo general or spinal anesthesia:
- Men with controlled but significant cardiac conditions previous MI, stents, heart failure
- Patients on warfarin, apixaban, rivaroxaban, or other anticoagulants
- Men with severe COPD where anaesthesia risk is elevated
- Older patients over 80 where surgical risk is prohibitive
- Patients with poorly controlled diabetes
For this group, who are frequently told they are not surgical candidates and are therefore left on medication indefinitely, PAE offers a definitive treatment option that surgery cannot safely provide.
Can PAE Be Done If You Are Currently on a Urinary Catheter?
Yes, and this is one of the most important clinical applications of PAE.
Men who have experienced acute urinary retention and are catheter-dependent are often told their only option is immediate surgery. PAE can be performed in catheter-dependent patients and in many cases allows catheter removal within 4 to 6 weeks as the prostate shrinks and urinary function restores.
This is a meaningful quality of life intervention for men who have been living with an indwelling catheter for weeks or months.
Key Takeaway: PAE has no upper prostate size limit, is specifically designed for high-surgical-risk patients, and can be performed in catheter-dependent men. These are the three patient groups most likely to be told they have limited options and for whom PAE most changes the clinical picture.
Recovery Timeline: What to Expect After PAE
Same-Day Discharge Protocol
Day of procedure:
- 2 to 4 hours monitored recovery after the catheter is removed
- Mild pelvic pressure and urinary frequency expected as inflammatory response begins
- Oral pain relief sufficient for most patients
- Discharged same day in the majority of cases
- Can eat and drink normally immediately
- A companion is required for travel home; no driving same day
Days 1 to 3:
- Urinary symptoms may temporarily worsen before improving; this is the post-embolization inflammatory response and is normal
- Increased urinary frequency and mild urgency for 48 to 72 hours
- Mild lower abdominal discomfort managed with oral analgesia
- Desk work resumes day 2 to 3 for most patients
Week 1 to 2:
- Urinary frequency begins improving
- Flow rate gradually increases as prostate begins reducing in volume
- Night-time waking episodes start reducing; most patients notice this first
- Energy levels are normal, no anaesthesia recovery fatigue
Timeline of Symptom Improvement
PAE results are not immediate. The prostate shrinks gradually as blood supply reduces.
| Timeframe | Expected Changes |
| Week 1–2 | Nocturia reduces first and most consistent early improvement |
| Week 2–4 | Urinary urgency decreases, leading to fewer emergency rushes |
| Month 1–2 | Flow rate measurably improves on uroflowmetry |
| Month 2–3 | Post-void residual decreases, and the bladder empties more completely |
| Month 3–6 | Maximum prostate volume reduction 20 to 40 percent typical |
| Month 6–12 | Symptom stability: IPSS scores plateau at improved level |
Long-Term Durability of PAE Results
Published long-term data shows:
- 5-year clinical success rates of 75 to 80 percent patients maintaining significant symptom improvement without further intervention
- Prostate volume reduction of 20 to 40 percent maintained at 5 years in responders
- A minority of patients approximately 15 to 20 percent require additional treatment within 5 years
- Repeat PAE is possible; unlike surgical revision, it carries no accumulated anatomical risk
- TURP remains available as a rescue option if PAE does not produce adequate response
A 2020 systematic review in European Urology comparing PAE to TURP found comparable symptom improvement scores at 12 months, with PAE demonstrating significantly superior sexual function preservation.
Key Takeaway: PAE produces sustained symptom improvement in 75 to 80 percent of patients at 5 years. Results build progressively over 3 to 6 months as prostate volume reduces. The first improvement most men notice is reduced night-time urination often within the first 2 weeks.
Consulting a Prostate Enlargement Specialist in Chennai
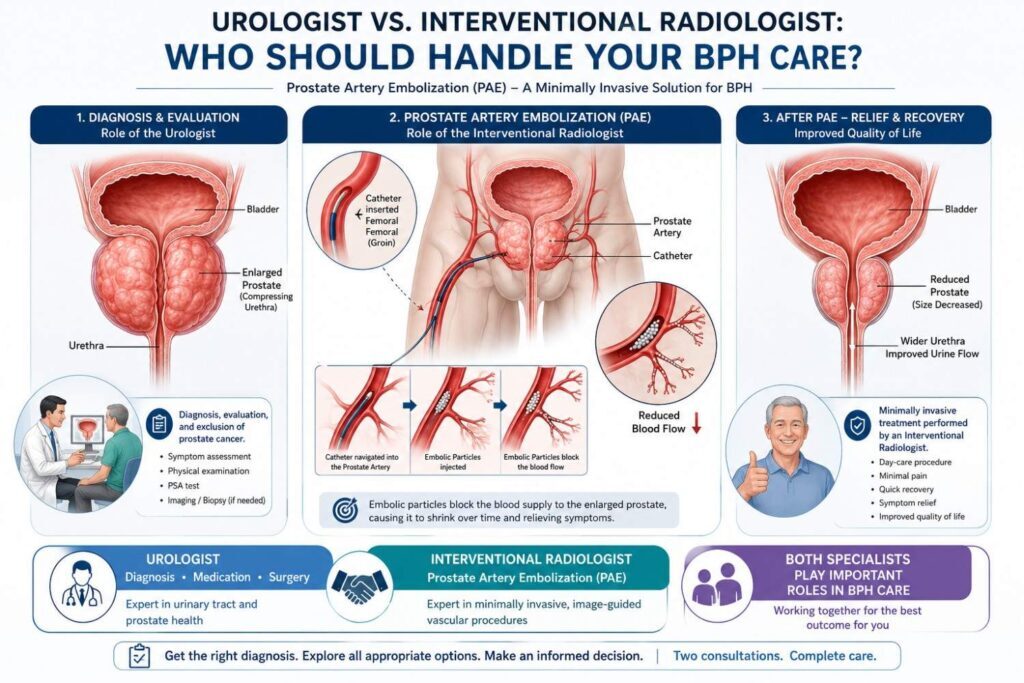
Urologist vs. Interventional Radiologist: Who Should Handle Your BPH Care?
Most men with prostate symptoms see a urologist first. This is appropriate: urologists diagnose BPH, rule out prostate cancer, manage medications, and perform surgical procedures.
But urologists do not perform PAE. PAE is a catheter-based procedure requiring interventional radiology expertise, DSA imaging capability, and microcatheter skills. It sits entirely within the specialty of interventional radiology.
The practical implication:
If you see only a urologist, you will be presented with urological options: medication, TURP, HoLEP, or open surgery. PAE will not typically be offered because it is not performed by urology. This is not negligence; it is a specialty boundary.
What this means for patients:
- Get your diagnosis and cancer exclusion from a urologist; this is essential
- Once BPH is confirmed and cancer excluded, request a referral to or direct consultation with an interventional radiologist for PAE assessment
- The two consultations take a combined total of 2 to 3 hours and give you the complete picture before any treatment decision
Advanced PAE at Dr. Ravindran’s IR Clinic in Chennai
For men in Chennai searching for the best treatment for an enlarged prostate without surgery or specifically seeking prostate artery embolization, the consultation starts with an interventional radiologist.
Dr Ravindran, an endovascular and interventional radiologist at Maruti Scans and Labs, at Veejay Towers, Velachery, Chennai, performs PAE as a dedicated outpatient procedure. Every case begins with an MRI or TRUS assessment to confirm prostate size, anatomy, and PAE suitability. IPSS score and uroflowmetry establish the baseline for outcome measurement.
The principle at Idoctor is consistent: surgery is always the last option. For men with BPH where a procedure exists that achieves comparable urinary outcomes without urethral instrumentation, without general anesthesia, and without retrograde ejaculation, that principle has the strongest possible clinical justification.
Key Takeaway: A urologist diagnoses BPH and excludes cancer. An interventional radiologist performs PAE. You need both consultations to make a genuinely informed treatment decision. If you have only seen a urologist, you have only seen half your options.
Frequently Asked Questions
A 2020 systematic review in European Urology found comparable IPSS symptom score improvement between PAE and TURP at 12 months. TURP achieves slightly better urine flow rates, but PAE produces equivalent symptom relief with zero retrograde ejaculation risk, same-day discharge, and local anesthesia only. For most men with moderate to severe BPH, the functional outcome difference is not clinically significant, but the sexual function preservation difference is dramatic.
PAE does not touch the urethra, the internal urethral sphincter, or the ejaculatory ducts. The retrograde ejaculation rate for PAE in published studies is less than 1 to 2 percent compared to 50 to 75 percent for TURP and 75 to 90 percent for HoLEP. Erectile function is also preserved in the vast majority of PAE patients. For sexually active men, this is the single most important reason to consider PAE before surgical alternatives.
The first improvement most patients notice is reduced night-time urination, often within the first 1 to 2 weeks. Daytime frequency and urgency improve over weeks 2 to 4. Flow rate improvement is measurable by months 1 to 2 as prostate volume reduces. Maximum symptom improvement typically occurs at 3 to 6 months when prostate shrinkage reaches its peak. Results continue to stabilize through the first year.
Yes to both. Very large prostates, over 80 grams, are particularly well-suited to PAE because their abundant arterial supply responds dramatically to embolisation. Blood thinners require careful peri-procedural management; anticoagulation protocols are adjusted around the procedure. Patients on warfarin, apixaban, or rivaroxaban are regularly treated with PAE with appropriate planning. These are two of the patient groups where PAE offers the clearest advantage over surgical alternatives.
Approximately 15-20% of PAE patients require additional treatment within 5 years. Repeat PAE is the first option; it carries no accumulated anatomical risk, unlike surgical revision. TURP or HoLEP remains fully available as a rescue option if PAE does not produce an adequate response. Choosing PAE first does not close off surgical options later. This is an important reassurance that PAE is a lower-risk first step that preserves all subsequent treatment pathways.
The Bottom Line
Prostate enlargement will not improve without treatment. It progresses. Year by year, the gland grows. The symptoms worsen. The risk of acute retention increases.
Medication manages symptoms without treating the cause. Surgery treats the cause but at the cost of general anesthesia, urethral instrumentation, and a 65 to 90 percent chance of permanent retrograde ejaculation.
PAE treats the cause without any of those trade-offs. Local anesthesia. Nothing through the urethra. Same-day discharge. Back to normal life in 5 to 7 days. Zero retrograde ejaculation risk. Comparable symptom relief to TURP at 12 months.
Every man with moderate to severe BPH deserves to know this option exists before signing a surgical consent form.
One PAE consultation. One MRI. Thirty minutes. The complete picture before you decide.
Book a prostate enlargement specialist consultation with Dr. Ravindran, interventional radiologist at Maruti Scans and Labs, at Veejay Towers, Velachery, Chennai.
+91 8190 907 908 | Learn About PAE

Comments are closed