PCN includes two closely related treatments:
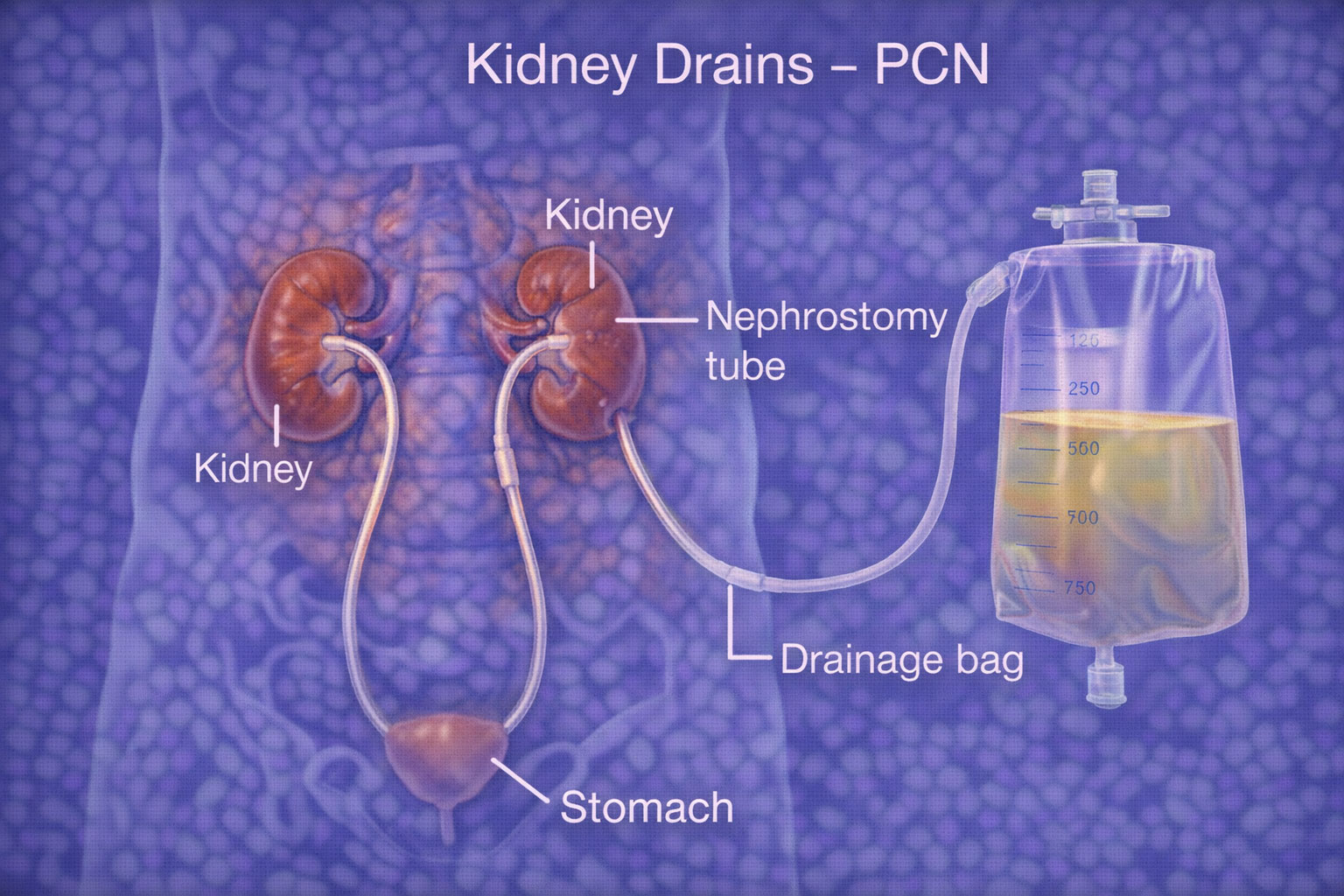
- Percutaneous nephrostomy: A small tube is placed through the skin into the kidney to drain urine outside into a bag.
- Ureteric stenting: A thin internal tube (stent) is placed from the kidney to the bladder to keep the urine pathway open.
This:
- Relieves pressure and pain
- Treats or prevents infection
- Protects kidney function
- Allows time for definitive treatment (stone removal, surgery, cancer therapy, etc.)
Understanding what is happening inside the kidney tissue itself is just as important as relieving the obstruction. A kidney biopsy is often performed in patients with longstanding obstruction to assess how much damage the kidney has sustained checking for scarring, inflammation, or irreversible injury that may affect how aggressively the kidney needs to be treated and whether full recovery of function is realistic after drainage is restored.
Obstruction is not the only reason a kidney can lose function. In some patients, the kidney is receiving insufficient blood supply because the renal artery — the main vessel feeding the organ has become narrowed. Renal artery angioplasty and stenting open this narrowed artery using a small balloon and stent delivered through a catheter, restoring adequate blood flow and often stabilizing kidney function in patients where poor circulation, rather than blockage, is the underlying problem.
Drainage procedures are not unique to the kidney. When bile cannot flow freely out of the liver due to a blockage in the bile duct caused by a stone, tumour, or stricture, a very similar technique is used. A biliary drain (PTBD) places a catheter through the skin into the bile duct under image guidance, relieving jaundice and infection in the same way that a PCN relieves urinary obstruction, making both procedures part of the same family of internal drainage solutions used across different organ systems.